

5 THINGS TO KNOW ABOUT SMOKING WEED WHILE PREGNANT & POSTPARTUM
- Use of cannabis by pregnant women has been growing in the USA in recent decades. A 2019 analysis of nearly half a million pregnant women in The National Institute on Drug Abuse found cannabis use more than doubled in the 15 years, between 2002 and 2017.
- Hard choices. A small study of pregnant women by Washington State University researchers found that women chose to use cannabis to avoid medications they felt were more harmful to their baby, such as anti-nausea pills, anti-psychotic medications and opioids. As with many things in cannabis, more research is needed. There’s little data about CBD combined with low amounts of THC.
- Breastfeeding. Data shows that on average, 10% of what you take in as cannabinoids will cross into breast milk for comparison, the amount of alcohol that crosses into breast milk is on average five to 6%.
- Topicals and CBD. Are CBD creams and patches totally different than smoking or vaping? Dr. Melanie Bone, OBGYN says not really. We often think of the skin as a barrier, but at the same time, the skin is the largest organ in the body and it does absorb a lot. And therefore to say, well, I’m just using a topical because I’m not ingesting it. And it’s not going through my liver as the first go or through my lungs, it should be safe.
- Quality. Cannabis purchased at licensed dispensary’s must pass rigorous state defined testing and regulation. CBD available for purchase nationally is not federally regulated.
KNOW THE FACTS ABOUT PREGNANCY & CANNABIS
With cannabis named an essential service, and the more open dialogue about its ability to reduce stress and anxiety, we know pregnant women are looking at weed more seriously than ever. So we also wanted to address a first of its kind research setting that was released after our original episode three aired.
This study details, the possible link between women smoking weed while pregnant and higher rates of autism in their children. In August of 2020 researchers from The Ottawa Hospital and affiliated institutions review data from every birth in Ontario, Canada from 2007 to 2012, which summed up to be more than a half a million women. Of those, 2200 women said they were smoking weed while pregnant without mixing it with tobacco, alcohol or opioids. The study found an association between maternal cannabis use and pregnancy and the incidence of autism spectrum disorder in the offspring.

SANDRA GUYNES, THE KUSH NURSE
HOW TO FIND THE BEST CANNABIS-FRIENDLY HEALTHCARE PROVIDER FOR YOU
“So I think the biggest thing is I always tell people, you, as a patient, if you’re pregnant or trying to have a baby and you are in a legal state, I would definitely try to find a provider that is comfortable with you using cannabis, if that’s what you want to do. And it’s hard to find those providers because they don’t have like a sign outside their door. But finding other moms that have gone through similar things is helpful and then interviewing your doctor, which sounds terrible but if you haven’t become pregnant yet, that’s the best time to interview those doctors and find out, “Are you comfortable with me using cannabis for XYZ purposes during my pregnancy?” And here’s the second thing. You may not have information about why or how your pregnancy outcomes will be using cannabis. However, if you’re using cannabis for a condition, you’re more likely to find studies, articles and supporting information about your condition to take to your provider.
And that’s always a good place to start because you can say, “I felt like this and with cannabis, I feel like this and my quality of life is better because X, Y, Z,” and now you have your own evidence to bring in. So sometimes it’s not necessarily saying like, “I want you to support my using it during pregnancy,” it’s saying, “I want you to support my condition because I’m a whole person with a baby inside of me that needs to manage these conditions.” And I think that’s really the part of advocating for yourself. It’s not just to say, “Hey, I want to use…” Because sometimes I think the doctors look at that as a personal decision. It is a personal decision, but it’s a medical decision also, it’s your body and your health.”
UNDERSTANDING ESTROGEN AND CANNABIS
Did you know that feeling effects of cannabis can be affected by your monthly hormones? A woman’s cannabis tolerance is inversely related to her estrogen level. Women are more responsive to the pain-relieving effects of cannabis and THC when estrogen levels are at their highest.
good to know
Cannabis influences fertility: THC appears to have the ability not only to inhibit ovulation but also prevent the implantation of fertilized eggs in the endometrium.
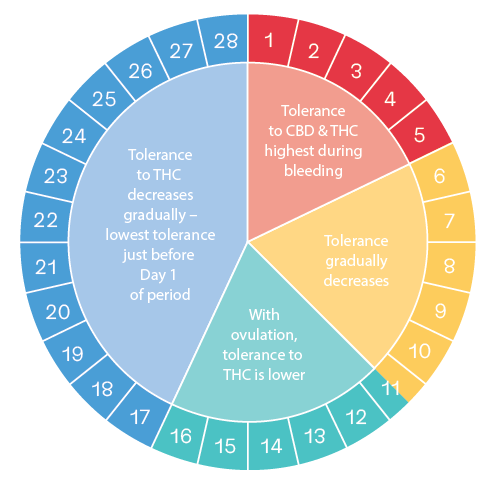

If you consumed during Days 1-12 and tolerated it well, you should reduce your dosage by ½ and build up.
WOMEN’S REPRODUCTIVE HEALTH, AGING + CANNABIS
A glossary to understand the stages of a woman’s reproductive health.
PREMENOPAUSE: Women still having periods and in reproductive years. Premenopausal women can develop a tolerance to THC quickly, and may be more vulnerable to negative side effects of cannabis such as paranoia, anxiety, or dependence.
PERIMENOPAUSE: Women still having periods but experiencing some symptoms of menopause. Boosting levels of endocannabinoids or stimulating cannabinoid receptors with cannabis may help delay menopause.
MENOPAUSE: Periods have stopped for one full year. Cannabis can support symptoms such as insomnia, vaginal dryness, mood swings caused by drops in estrogen levels.
POSTMENOPAUSE: Women may be able to stay on a stable dosage of THC or cannabis for the long-term, and may be less likely to feel anxious or paranoid from cannabis. Since menopausal and postmenopausal women have low levels of estrogen, they may be less responsive to THC and may require higher doses than premenopausal women to achieve the same amount of pain relief.
Any given month in a premenopausal woman’s cycle, your hormone levels fluctuate from the beginning to the end of that cycle. And so, of course, you have to realize that the way that we metabolize medication, the way that we respond to medication may be different at any given time. And that’s partly why women were left out of studies, because it was thought to be too costly to integrate women into those studies. It was much easier to do studies on pharmaceuticals and other entities using a male. – Dr. Colene Arnold, OB/GYN